Where does FGM/C occur?

What are the types of FGM/C?

Type I – Clitoridectomy:
Clitoridectomy refers to the partial or total removal of the externally visible part of the clitoris and/or the clitoral hood (prepuce).
This form is often mistakenly referred to as a "mild" type of FGM/C. However, this is misleading: the clitoris is a highly sensitive and complex organ. Its removal causes not only intense physical pain but can also result in lasting damage to sexual, physical, and emotional health.

Type II – Excision:
Excision involves the partial or total removal of the clitoris and the inner labia (labia minora). In some cases, the outer labia (labia majora) may also be cut or damaged.
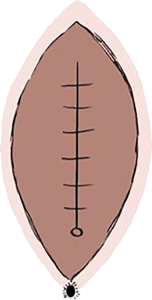
Type III – Infibulation:
Infibulation is considered the most severe form of FGM/C. It involves the removal of the clitoris and the labia, followed by stitching the vaginal opening closed, leaving only a small hole for urine and menstrual blood to pass through.
For sexual intercourse or childbirth, the opening must be surgically or manually reopened – and in many cases, it is sewn shut again afterward.
This practice causes lifelong physical and psychological trauma and represents a grave violation of bodily autonomy and human dignity.
Why is FGM/C performed?
What are the physical and psychological consequences of FGM/C?
Isn´t FGM/C forbidden?
